WHY FAT CONTENT DOESN’T REALLY MATTER
WHY FAT CONTENT DOESN’T REALLY MATTER
- Manage your Account
- Start Here
- Guides
- Nutrition
- Training
- Lifestyle & Motivation
- Webinars
- Research Reviews
- Resources
What you’re about to get into?
- 1200 words – 9 min read.
Key Points
- Dietary fat can increase blood glucose levels when consumed on its own. However,
- When dietary fat is consumed alongside carbohydrates and protein – the effect on blood glucose is more significant.
- Consume the bulk of your dietary fat from monounsaturated food sources and the least from highly processed food sources.
- Dietary cholesterol is not a nutrient of concern – stop panicking and eat foods that contain cholesterol in peace.
- Fat is incredibly easy to eat, especially when combined with carbohydrate, protein and salt.
- Be mindful that dietary fat can drive you into an energy surplus quicker than any other macronutrient.
In this article, I want to dispell the common fear most people have about the fat content of their foods and highlight the more important aspects people need to consider when chasing the goal of better health, body compsotion, sports performance and highly effective diabetes management.
Good and Bad Fats – Let’s Begin.
Before we get to the interesting stuff, I want to give a quick rundown on the different types of dietary fat.
Why?
Because not all fats are created equal.
Although the terms ‘Good / Bad’ Fats are quite subjective, it is generally agreed amongst scientists that the terms apply to the effects a certain type of fat has on cholesterol in the blood, more specifically, lipoproteins (the carriers of cholesterol).
Enter cholesterol a small waxy substance that serves many important roles within the body, including being an important component of every cell membrane in the body and playing a major role in tissue repair.
High-density lipoprotein (HDL) and Low-density lipoprotein (LDL) are the two main classifications of plasma lipoprotein particles and are dubbed “good” and “bad” cholesterol.
Respectively: LDL-Cholesterol is labelled as ‘bad’ due to its potential atherogenic properties.
When a blood vessel is damaged, LDL-Cholesterol is called upon to repair it. Depending on the extent of the damage, fatty deposits can appear on the walls of the blood vessels (known as plaque). These plaques (or atheromas) are known as atherosclerosis and cause the arteries to harden and narrow, restricting the blood flow and oxygen supply to vital organs.
However, just because LDL-Cholesterol is correlated to the formation of plaque and furrowing of the arteries does not mean it caused the damage in the first place.
Damage to blood vessels is increased by a number of risk factors, including:
- Obesity (metabolic syndrome and T2)
- Poor glycaemic control
- Genetic predisposition
- Excessive intake of man-made trans-fat
- Smoking
- Oxidative stress
- Low-grade inflammation ( other illness etc.)
- Chronic stress
Generally speaking, the distinction between ‘good’ and ‘bad’ cholesterol is valid, making further distinctions beyond the scope of this article.
Cholesterol – Correlation Doesn’t Equal Causation.
A Short Primer on The Effect of Different Dietary Fats
Dietary fats, technically speaking, triglycerides, are made up of one molecule of glycerol (a sugar) and three fatty acids.
I don’t want to go into a whole biochemistry lesson on the structure of fatty acids in this article; however, it is important to know that the effects of fatty acids on health and metabolism depend primarily on their structure.
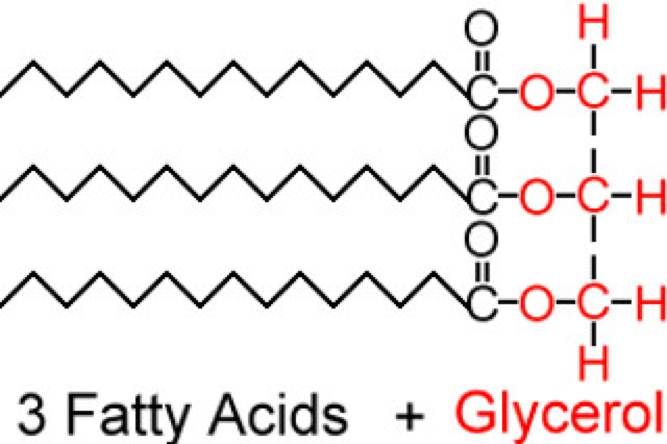
Picture of a Triglyceride Molecule
Triglycerides can differ in length, from short to medium to long chain (depending on the number of carbons present), and by the number of double bonds. There are four main subtypes of dietary fat/triglycerides.
Trans Fats
Man-made trans-fatty acids AKA partially hydrogenated vegetable oils, occur mainly in margarine and junk food to give them long shelf lives.
The consumption of industrially produced, partially hydrogenated vegetable oils (trans fat) is associated with an increased risk of cardiovascular disease, infertility, endometriosis, gallstones, Alzheimer’s disease, diabetes and some cancers.
Thankfully, many fast-food and supermarket chains have either considerably reduced, or eliminated the use of these types of fats in their food.
The intake of trans fat is relatively low in the UK and northern Europe. It tends to be consumed in greater quantities in other countries, particularly the United States. Be mindful of this when travelling.
The 2015-2020 Dietary Guidelines for Americans recommends trans fat should be avoided.
There is nothing good to come out of eating man-made trans fats. They are one of the only sources of fat that should be avoided.

Saturated Fats
The type of fat most will be familiar with.
Saturated fat is solid at room temperature, has no double bonds and occurs predominantly in animal foods, such as meat, eggs, dairy products and certain plant products like coconut oil.
The hysteria surrounding saturated fat has worn off since the 1980s as it then became sugar’s turn to take a bashing.
Check this article out after The Truth: Is Sugar Addictive?
Saturated fats are not essential to have in the diet. Our bodies can create saturated fat from excess carbohydrate and protein.
The 2015-2020 Dietary Guidelines for Americans recommends people limit saturated fat to less than 10% of calories a day.
Though there are many types of saturated fats, they tend to increase both HDL (good) and LDL (bad) cholesterol. As the ratio of HDL to LDL is more important than the quantity of each, they are pretty neutral with respect to health in most instances.
That said, at low doses saturated fats are acceptable in our diets and not atherogenic (promoting the formation of plaque in the arteries). However, if you consume the bulk of your fat intake from saturated fats, particularly palmitic acid (commonly found in butter), you may dramatically increase your risk of developing atherosclerosis.
So, if your fat intake largely consists of cream, butter, lard and other saturated goodness – you might be as well to start incorporating the following sources of fat, as of today…
![Diabetes, Bacon and Eggs [50%] [50%]](https://diabeticmuscleandfitness.com/wp-content/uploads/2017/10/Diabetes-Bacon-and-Eggs-50-50.jpg)
Monounsaturated Fats
Monounsaturated fats are liquid at room temperature, have a single double bond and occur predominantly in foods like olive oil, nuts, and seeds.
In terms of health, monounsaturated fats are neutral to beneficial, as they tend to reduce levels of LDL in the blood.
As such, monounsaturated fats should make up the bulk of your fat intake.
Saturated fats can also be replaced by monounsaturated fatty acids, which are considered health-neutral, provided they are consumed within an individual’s energy needs and consumed as part of a diet that provides all the necessary essential nutrients. This is often considered to be a Mediterranean diet.

Polyunsaturated Fats
Polyunsaturated fats are also liquid at room temperature and have multiple double bonds.
The two primary classes of these fats are the essential omega-3 and omega-6 fatty acids.
The body cannot produce omega-3 and omega-6 fatty acids. For this reason, they are known as essential fats or EFAs.
Omega-3 helps to reduce inflammation; omega-6 promotes inflammation, which at times is healthy and essential for human growth, development and repair.
While both of these fats are essential…
Chronically high levels of Omega-6, at the expense of Omega-3, have been shown to promote inflammation and contribute to modern diseases, such as heart disease, obesity and diabetes.
Omega-6 is hard to avoid considering everything is cooked in some form of vegetable oil – the most popular source of omega-6 fatty acids.
Most people could benefit from increasing their omega 3 intakes, particularly from animal sources – which tend to be higher quality over plant-based sources.
- Strive to eat eight or more ounces (226g) a week from a variety of oily seafood.
- The American Heart Association recommends 1g daily. If the goal of supplementation is to reduce soreness, a 6g dose, spread over the course of a day, will be effective.
Plant sources such as flaxseed, chia, hempseed, canola oil, walnuts and certain vegetable oils contain significant amounts of the plant-based omega-3 fatty acid A-linolenic acid (ALA) and stearidonic acid (SDA).
Animal sources, particularly fish/krill oil and oily fish contain the omega-3 fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA)
Researchers now believe that the majority of health benefits we get from dietary omega-3 fats come from EPA/DHA, particularly DHA. They carry just about any positive health effect you can think of.

Does Fat Content Really Matter?
Fat content is important.
However, we rarely eat dietary fat on its own.
When was the last time you chugged down a bottle of olive oil or ate a pound of lard pre-workout?
Never?
Thought so.
We consume 99% of our dietary fat alongside other nutrients – other foods.
Pure fat sources like olive oil and butter are traditionally consumed with bread, salad and other nibbles.
Cooking oils are the foundation of pretty much every dish on the planet.
The only exceptions to this – is when we eat pure dietary fat, such as…
- Supplementing with fats like cod liver or flaxseed oil.
- Falling prey to crazy pseudoscience nonsense like bulletproof coffee or the whole ‘coconut oil is good for me’ craze.
Food choice matters most, not the fat content.
Even your favourite peanut butter (a source of fat) or a certain variety of nuts contain their fair share of carbs and protein.
The concept Food choice matters most, not the fat content is supported by the relatively new recommendations on dietary fat set by the U.S. Department of Health and Human Services Dietary Guidelines Advisory Committee, which states…
There is no longer a recommended upper limit for total fat intake.
There really is no scientific basis for placing a limit on fat intake, with the exception of avoiding man-made trans fats.
In fact, fearing fat can encourage poor dietary choices.
For example, restricting dietary fat may hinder an individual from consuming foods rich in healthy fats, like salmon, mackerel and avocados which pack significantly more nutritional value than popular dietary foods like rice cakes or artificially processed dressings, deli meats, confectionery and ready meals with ‘fat-free claims.’
No more freaking out about the total fat content of your food. Shift your focus to food choice.
Rather than worrying about the type of fat you are eating, consider asking yourself more important questions like.
- What quantity and other types of nutrients am I eating alongside the dietary fat in my meal?
- Does my meal/food portion sit within or outside my calorie targets for my particular body composition goals?
- Will this fill me up? or leave me hungry and wanting more calories?
- How will my blood glucose levels respond to the fat content in this food/meal?
- Are there any additional nutrients that accompany the fat source, e.g Protein, Carbs, Vitamins and Minerals?
Failing to ask these questions will likely lead to body composition issues and problems with managing blood glucose levels.
Look beyond the fat!
Take Home
- Dietary fat promotes the secretion of insulin in people without diabetes.
- For those living with diabetes, dietary fat has the potential to increase blood glucose levels. Dose and frequency specific.
- Dietary fat has the most insignificant impact on blood glucose levels when compared to carbohydrate and protein alone.
- Consume the majority of your dietary fat from monounsaturated sources, with the rest split between saturated and polyunsaturated fats.
- Consume as little man-made trans fatty acids as possible.
- Though the quantity and types of fat that you consume on a daily basis are certainly a key factor in optimising health, it is important to realize that other dietary and lifestyle factors are far more important.
References
Written by Phil Graham
Founder of Diabetic Muscle and Fitness
Sports Nutritionist, Strength Coach, and Fitness Educator
Type 1 Diabetic for 12 years